打开文本图片集
[摘要] 目的 探讨心肌损伤标志物检测在新生儿缺氧缺血性脑病(HIE)严重程度评估中的价值。 方法 采用病例-对照研究,选取本院2014年5~10月的271例HIE患儿,根据新生儿HIE诊断标准分为重度72例、中度86例、轻度113例,并以同期120例健康新生儿作为健康对照组,用全自动化学发光免疫分析法动态检测各组血清心肌肌钙蛋白I(cTnI)、肌红蛋白(Myo)和肌酸激酶同工酶(CK-MB)浓度,统计分析心肌损伤标志物变化与脑损伤的关系。 结果 患病12~24 h,cTnI以重度HIE组最高,为(1.56±1.33)μg/L;中度、轻度HIE组次之,分别为(0.63±0.47)、(0.26±0.17)μg/L,均明显高于健康对照组 [(0.06±0.05)μg/L] (F=97.64,P<0.01)。271例HIE患儿心肌损伤发生率为40.96%,其中重度HIE组为87.50%,中度HIE组为46.51%,轻度HIE组为7.08%,3组比较差异有统计学意义(χ2=119.22,P<0.01)。患病12 h内,重度、中度、轻度HIE组3种心肌损伤标志物均以Myo异常率最高;患病12~24 h,HIE各组cTnI、Myo、CK-MB异常率基本一致;患病2 d后,HIE各组Myo异常率均持续下降,cTnI和CK-MB异常率却维持在较高水平达5~8 d。 结论 HIE患儿心肌损伤与脑损伤紧密相联——脑损伤越重,心肌损伤也越重;检测心肌损伤标志物有助于HIE严重程度的评估。
[关键词] 新生儿缺氧缺血性脑病;心肌肌钙蛋白I;肌红蛋白;肌酸激酶同工酶
[中图分类号] R722.1 [文献标识码] A [文章编号] 1674-4721(2015)08(c)-0132-04
[Abstract] Objective To investigate the value of myocardial damage markers in the severity assessment of hypoxic ischemic encephalopathy (HIE) in neonates. Methods Case-control study was used,and 271 cases with HIE from May to October 2014 in our hospital were selected.According to the diagnostic criteria for HIE in neonates,the patients were divided into severe ones (72 cases),moderate ones (86 cases) and mild ones (113 cases).120 healthy neonates were selected as healthy control group at the same time.The concentration of serum cardiac troponin I (cTnI),myoglobin (Myo) and creatine kinase isoenzyme MB mass (CK-MB) were dynamically detected by fully automatic chemiluminescence immunoassay.The relationship between the change of myocardial damage marker and brain damage was statistically analyzed. Results When sick for 12 to 24 hours,the concentration of three HIE groups were higher when compared with healthy control group [(0.06±0.05) μg/L].The concentration of cTnI was the highest in severe HIE group [(1.56±1.33) μg/L],the secondly higher in moderate HIE group [(0.63±0.47) μg/L] and the thirdly higher in mild HIE group [(0.26±0.17) μg/L] (F=97.64,P<0.01).The incidence rate of HIE myocardial damage was 40.96%.Among them,the percentage in severe HIE group was 87.50%,in moderate HIE group was 46.51% and in mild HIE group was 7.08%,and there was significant difference among them (χ2=119.22,P<0.01).When sick less than 12 hours,abnormal rate of Myo was the highest in the three kinds of myocardial damage markers in the severe,moderate and mild HIE group.When sick for 12 to 24 hours,abnormal rate of cTnI,Myo and CK-MB in three HIE groups were basically consistent.When sick more than 2 days,abnormal rate of Myo in three HIE groups continued to decrease.And the abnormal rates of cTnI and CK-MB were maintained at a higher level for 5 to 8 days. Conclusion There is a close association between myocardial damage in neonates with HIE and brain damage—the more serious the brain damage of HIE newborns,the more serious the myocardial damage is.The detection of myocardial damage marker is helpful to the assessment of the HIE severity.
[Key words] Hypoxic ischemic encephalopathy in neonates;Cardiac troponin I;Myoglobin;Creatine kinase isoenzyme MB
新生儿缺氧缺血性脑病(hypoxic ischemic encephalopathy,HIE)是指围生期窒息导致脑的缺氧缺血性损害,临床可分重、中、轻度,脑组织以水肿、软化、坏死和出血为主要病变,临床主要表现为意识障碍、脑水肿、惊厥、肌张力变化、原始反射异常等一系列中枢神经系统的异常[1]。围生期窒息是本症的主要病因,缺氧缺血是本症的重要本质[2],缺氧不仅可导致新生儿脑损伤,而且因呼吸循环功能不良,可引起心肌功能障碍[3-4]。为探讨HIE心肌损伤与脑损伤的关系,本研究检测了72例重度HIE、86例中度HIE、113例轻度HIE患儿血清心肌肌钙蛋白I(cTnI)、肌红蛋白(Myo)和肌酸激酶同工酶(CK-MB)3种心肌损伤标志物的浓度,并以120例健康新生儿作为对照,现报道如下。
1 资料与方法
1.1 一般资料
选取2014年5~10月在本院住院的HIE患儿271例,根据新生儿缺氧缺血性脑病诊断标准[5],诊断重度72例(61例痊愈、8例好转、3例死亡),中度86例(83例痊愈、3例好转),轻度113例(全部痊愈);男143例,女128例,胎龄(38.53±1.72)周;剖宫产145例,产道分娩126例。健康对照组120例,男64例,女56例,胎龄(39.11±1.65)周;剖宫产67例,产道分娩53例。HIE组与健康对照组的胎龄、男女构成比、分娩方式比较,差异均无统计学意义(P>0.05),具有可比性。
1.2 材料
1.2.1 仪器 Siemens ADVIA Centaur XP全自动化学发光免疫分析仪(美国,西门子公司)。
1.2.2 3种心肌损伤标志物试剂、校准品 美国西门子公司配套产品。
1.2.3 3种心肌损伤标志物质控品 伯乐生命医学产品(上海)有限公司产品。①低值质控品(批号23551)cTnI为(0.06±0.01)μg/L、Myo为(69.09±4.51)μg/L、CK-MB为(3.28±0.20)μg/L;②高值质控品(批号23553)cTnI为(9.65±0.90)μg/L、Myo为(303.24±20.00)μg/L、CK-MB为(50.16±2.52)μg/L。
1.3 样品检测与结果判断
真空采血管采集HIE患儿<12 h、12~24 h、2~4 d、5~8 d、9~14 d静脉血,对照者采集12~24 h静脉血,1 h内分离血清,用Siemens ADVIA Centaur XP全自动化学发光免疫分析仪测定cTnI、Myo、CK-MB浓度,操作严格按标准操作程序执行,所有质控结果均在控。cTnI、Myo、CK-MB分别以>0.10、>110.00、>5.00 μg/L为升高。
1.4 统计学处理
所有数据用SPSS 16.0 统计学软件处理,计量资料用x±s表示,多组间比较采用One-way ANOVA 分析,当P<0.05 时再进行两组间比较的SNK-q检验;计数资料用百分率表示,采用 χ2 检验,多个样本率间的两两比较用卡方分割法[6],以P<0.05 为差异有统计学意义。
2 结果
2.1 HIE组与健康对照组心肌损伤标志物检测结果的比较
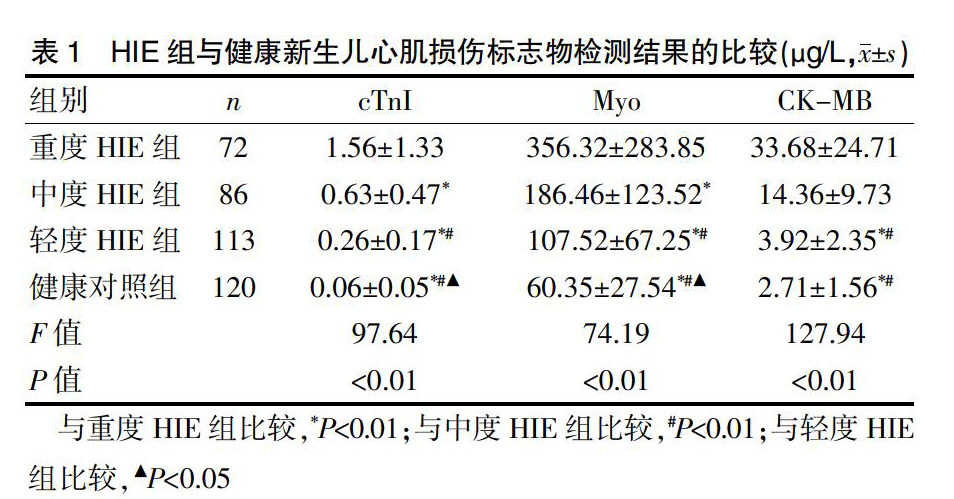
患病12~24 h,cTnI、Myo均以重度HIE组最高,中度、轻度HIE组次之,均明显高于健康对照组(P<0.01);CK-MB以重度HIE组最高,中度HIE组次之,明显高于轻度HIE组、健康对照组(P<0.01),而轻度HIE组与健康对照组的CK-MB比较,差异无统计学意义(q=0.92,P>0.05)(表1)。
2.2 HIE患儿心肌损伤发生率及不同住院时间心肌损伤标志物异常率
271例HIE患儿心肌损伤发生率为40.96%(111/271),其中重度HIE组为87.50%(63/72),中度HIE组为46.51%(40/86),轻度HIE组为7.08%(8/113),3组比较差异有统计学意义(χ2=119.22,P<0.01)。患病<12 h内,重度、中度、轻度HIE组3种心肌损伤标志物均以Myo异常率最高;患病12~24 h,HIE各组cTnI、Myo、CK-MB异常率基本一致;患病2 d后,HIE各组Myo异常率均持续下降,cTnI和CK-MB异常率却维持在较高水平达5~8 d(表2)。
3 讨论
HIE是指由各种原因引起的缺氧和脑血流量减少而导致的新生儿脑损伤,患儿常在患病后1周尤其头3 d内出现一系列脑功能障碍表现,如烦躁不安或嗜睡、吐奶、尖叫、抽搐等症状,轻症患者预后良好,病情危重者,病死率高,幸存者可留下后遗症,如脑性瘫痪、智力低下、癫痫、耳聋、视力障碍等[7-8]。本组72例重度HIE患儿3人死亡,死亡率达4.17%,可见本病严重威胁着新生儿的生命和健康。
新生儿HIE心肌损伤是HIE常见的并发症[9-10],HIE发生后因心肌缺血缺氧,心肌细胞能量代谢障碍,糖无氧酵解增加导致酸性代谢产物蓄积,细胞内酸中毒,使细胞膜结构破坏、通透性增加,细胞内cTnI、Myo、CK-MB释放入外周血使其浓度升高[11]。本组HIE组患病12~24 h,cTnI、Myo均以重度HIE组最高,中度、轻度HIE组次之,均明显高于健康对照组(P<0.01);CK-MB以重度HIE组最高,中度HIE组次之,明显高于轻度HIE组和健康对照组(P<0.01)。HIE患儿心肌损伤发生率为40.96%,其中重度HIE组为87.50%,中度HIE组为46.51%,轻度HIE组为7.08%,3组比较差异有统计学意义(P<0.01),说明HIE患儿心肌损伤与脑损伤紧密相联,脑损伤越重,心肌损伤也越重,检测心肌损伤标志物有助于HIE严重程度的评估,有利于及早采取相应的医疗措施。
临床上用于诊断心肌损伤的标志物主要有Myo、cTnI和CK-MB[12]。Myo主要分布于心肌和骨骼肌中,是心肌损伤6 h内目前较好的早期标志物,在心肌受损后2~3 h即可出现在外周血中,峰值在疾病发生后6~9 h出现,阳性持续时间短[13]。cTnI是心肌纤维上专有的收缩蛋白,其绝对的心肌特异性完全可以区分心肌和骨骼肌的损伤,是目前诊断心肌损伤特异度最强和灵敏度较高的标志物[14-15],当心肌损伤4 h后,cTnI开始在血液中升高,阳性持续时间长[16]。CK-MB是CK 3种组织同分异构形式之一,主要位于心肌细胞中,当心肌细胞损伤后释放进入外周血,在12 h达峰值[17-18]。在临床观察、了解心肌损伤后有无再损伤或损伤区域有无扩大时,Myo或CK-MB是较好的标志物。
本研究结果显示,患病12 h内,重度、中度、轻度HIE组3种心肌损伤标志物均以Myo异常率最高;患病12~24 h,HIE各组cTnI、Myo、CK-MB异常率基本一致;患病2 d后,HIE各组Myo异常率均持续下降,cTnI和CK-MB异常率却维持在较高水平达5~8 d,提示动态检测心肌损伤标志物,有助于HIE患儿心肌损伤的早期诊断、疗效评估及预后判断。
[参考文献]
[1] Tagin MA,Woolcott CG,Vincer MJ,et al.Hypothermia for neonatal hypoxic ischemic encephalopathy:an updated systematic review and meta-analysis[J].Arch Pediatr Adolesc Med,2012,166(6):558-566.
[2] Gulczyńska E,Gadzinowski J.Therapeutic hypothermia for neonatal hypoxic-ischemic encephalopathy[J].Ginekol Pol,2012,83(3):214-218.
[3] Beken S,Ayd"n B,Dilli D,et al.Can biochemical markers predict the severity of hypoxic-ischemic encephalopathy? [J].Turk J Pediatr,2014,56(1):62-68.
[4] Sweetman D,Armstrong K,Murphy JF,et al.Cardiac biomarkers in neonatal hypoxic ischaemia[J].Acta Paediatr,2012, 101(4):338-343.
[5] 中华医学会儿科学分会新生儿学组.新生儿缺氧缺血性脑病诊断标准[J].中华儿科杂志,2005,43(8):584.
[6] 黄水平.多个样本率间的两两比较方法[J].徐州医学院学报,2002,22(4):291-294.
[7] Buonocore G,Perrone S,Turrisi G,et al.New pharmacological approaches in infants with hypoxic-ischemic encephalopathy[J].Curr Pharm Des,2012,18(21):3086-3100.
[8] Selway LD.State of the science:hypoxic ischemic ence-phalopathy and hypothermic intervention for neonates[J].Adv Neonatal Care,2010,10(2):60-66.
[9] Hochwald O,Jabr M,Osiovich H,et al.Preferential cephalic redistribution of left ventricular cardiac output during therapeutic hypothermia for perinatal hypoxic-ischemic encephalopathy[J].J Pediatr,2014,164(5):999-1004.
[10] Shastri AT,Samarasekara S,Muniraman H,et al.Cardiac troponin I concentrations in neonates with hypoxic-ischaemic encephalopathy[J].Acta Paediatr,2012,101(1):26-29.
[11] Simovi AM,Igrutinovi Z,Obradovi S,et al.The significance of second generation cardiac troponin I in early screening of hypoxic-ischemic encephalopathy after perinatal asphyxia[J].Srp Arh Celok Lek,2012,140(9-10):600-605.
[12] 杨振华,潘柏申,许俊堂.中华医学会检验学会文件心肌损伤标志物的应用准则[J].中华检验医学杂志,2002, 25(3):185-189.
[13] Sonobe T,Akiyama T,Du CK,et al.Contribution of calpain to myoglobin efflux from cardiomyocytes during ischaemia and after reperfusion in anaesthetized rats[J].Acta Physiol (Oxf),2014,210(4):823-831.
[14] Bohula May EA,Bonaca MP,Jarolim P,et al.Prognostic performance of a high-sensitivity cardiac troponin I assay in patients with non-ST-elevation acute coronary syndrome[J].Clin Chem,2014,60(1):158-164.
[15] Sandoval Y,Smith SW,Schulz KM,et al.Diagnosis of type 1 and type 2 myocardial infarction using a high-sensitivity cardiac troponin I assay with sex-specific 99th percentiles based on the third universal definition of myocardial infarction classification system[J].Clin Chem,2015, 61(4):657-663.
[16] Barbier CE,Themudo R,Bjerner T,et al.Cardiac troponin I associated with the development of uecognized myocardial infarctions detected with MRI[J].Clin Chem,2014, 60(10):1327-1335.
[17] 刘成桂.急性冠脉综合征心肌损伤和易损斑块生化标志物检测进展[J].四川医学,2008,29(7):932-934.
[18] Baydin A,Amanvermez R,Tuncel ?魻K,et al.Ischemia-modified albumin is not better than creatine kinase-MB and cardiac troponin I in predicting a cardiac injury in nontraumatic subarachnoid hemorrhage[J].Am J Emerg Med,2015,33(4):488-492.
(收稿日期:2015-04-21 本文编辑:许俊琴)
扩展阅读文章
推荐阅读文章
花田文秘网 https://www.huatianclub.com
Copyright © 2002-2018 . 花田文秘网 版权所有